To help residents and young radiologist learn the use of thoracic ultrasound is necessary to know the basic ultrasound physics and the normal pulmonary signs.
Reverberation artifacts
The reverberation artifact is an horizontal or vertical image that occurs when ultrasound waves bounce between two interfaces with high acoustic impedance (pleura or interlobullar septae).
The waves moves up and down between these interfaces and the machine recognise them as parallel lines which have equal distances between them.
This artefact known as “A lines” represents multiple parallel lines horizontal hyperechogenic lines beneath the pleural line.
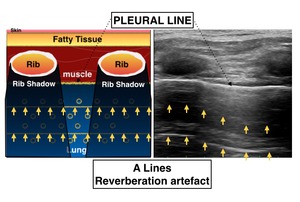
Fig. 1: "A Lines"
B lines: are narrow based hyperecogenic lines with a vertical orientation,
that arise from the pleural line and extends to the edge of the ultrasound screen.
This artifact is also know as “comet-tail artifacts”.
B lines artifact can be seen in normal patients with a 7 mm distance spacing.
(normal spacing of the interlobular septae)
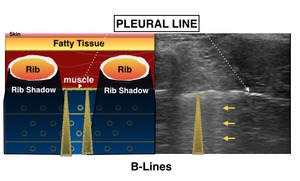
Fig. 2: "B Lines"
Z lines: It may represent like the B lines but not to be confused with these lines,
because Z lines doesn’t reach distally to the edge of the screen.
Found in patients with no pathology,
as well as in patients with pneumothorax.
They are less echogenic than the pleural line,
and they diminish between 2-4 cms.
Also this artifact doesn’t erase “A lines,
and do not move with lung sliding.
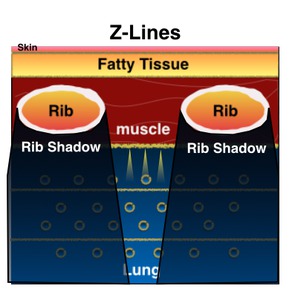
Fig. 3: "Z Lines"
E lines: Comet tail artifact seen in superficial and superior the pleural line in patients with parietal emphysema or echogenic foreign bodies in the chest wall.
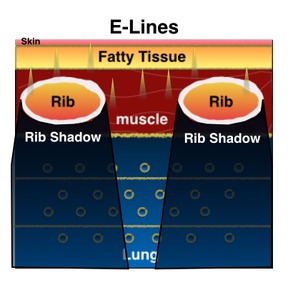
Fig. 4: "E Lines"
Normal Findings Bedside Thoracic Ultrasound.
Bedside ultrasound strict decontamination protocol in each given procedure.
The probe can be a convex probe 1-5MHZ or a Linear probe 7-15 MHZ.
Always use a systematic and dynamic approach to obtained and interpret the ultrasound images.
Also describe the position of the patients (supine,
decubitus lateral,
etc),
as well as the area of examination with the help of diagram probe positioning that every ultrasound machine has.
The probe should be positioned perpendicularly between the ribs in a longitudinal orientation.
Left side of the screen (ultrasound mark) should always point cephalic positioning,
and the right side of the screen should correspond to caudal part
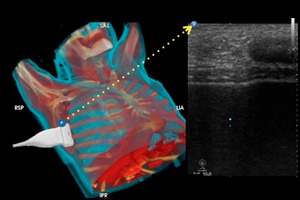
Fig. 12
Thoracic ultrasound examination
Divide the thorax into Upper and lower segments in each hemithorax.
Also divide each segment into 4 zones.
These áreas should be explore systematically which should take less than 5 minutes using both probes.
Linear probe (7-15 Mhz) has a better definition image to detect pneumothorax but has a weak ultrasound wave penetration were the convex probe (2-5 Mhz) helps to detect posterior defects.
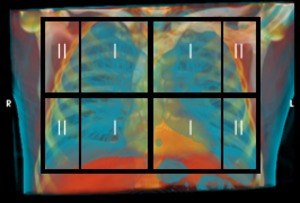
Fig. 5: Anterior View of Thoracic Zones.
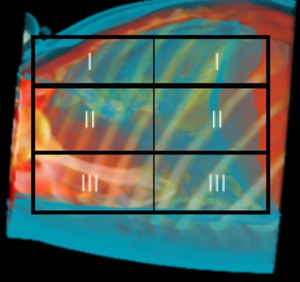
Fig. 6: Lateral View of Thoracic Zones
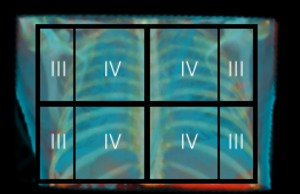
Fig. 7: Posterior View of Thoracic Zones
ICU patients tend to be critical ill,
so thoracic ultrasound examination can be very difficult.
Zone 4 is a difficult zone to examine because patients ,
but pneumothorax (free air between visceral and parietal pleura) usually moves freely to the most upper part of the thorax depending of the situation of the patient (supine).
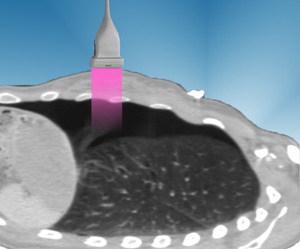
Fig. 8: Diagram (parasagittal thoracic CT) illustrating thoracic ultrasound detecting an anterior pnemothorax that usually locates in the most anterior and superior part of the thorax, studied in a supine position.
However thoracic ultrasound can detect smaller pneumothoraces compared with conventional chest radiography done with portable X-ray units.
Ultrasound signs in normal healthy patients
Lung Sliding
The visual appearance of the pleural movement (viewed in the 2D-mode or B-mode) in every breath the patient takes or the tidal movement done by the mechanical ventilator if the patient is intubated.
The pleural line is made up of the visceral and parietal pleura surfaces.
During respiration,
the two pleural surfaces slide against each other (air displacement),
and this appears as a shimmering white line.

Fig. 14
Seashore sign
M-mode is an effective tool with the ultrasound to detect movement,
with a very sensitive and especificity to detect small pneumothorax.
It's called seashore sign because it resembles a sky,
ocean and beach.
It is important to notice the beach part or the grainy part,
because grain represents pleural movement.

Fig. 10

Fig. 13
The beach part in the image is obtained by the motion detected by the sliding effect of the pleura.
When no movement is detected a A line pattern appears in which it resembles a sky or sunset called:
-Strathosphere Sign--> Pneumothorax.
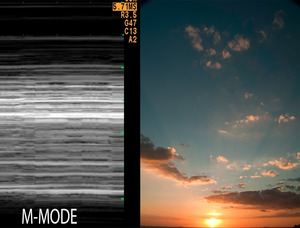
Fig. 11
Power slide
Using the B-mode in the ultrasound and the power doppler it can easily detect the pleural movement with a laminar enhacement in the power doppler signal located in the pleural line.
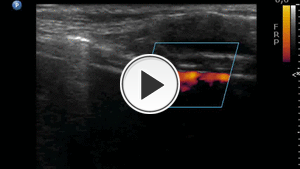
Fig. 15
How to detect pneumothorax
Abscence of lung sliding
No movement is present between the pleural line with a normal patient breathing (several respiratory cycles).
"A-lines" can be present in pneumothorax because A means Air so you can remember.
But "B-lines" which are reverberation artifacts obtained by interlobullar septae thickening,
so B-lines doesn't diagnose pneumothorax.
Strathosphere sign
Strathosphere sign is obtained with the M-mode observed through the pleural line between the ribs with several respiratory cycles.
False positive strathosphere sign can be detected in COPD patients with small breathing movement.
It is important to focus on all the thoracic zones described previously,
and to ask the patient to breath heavily like a normal clinical examination is performed.
If the patient is critical ill with traqueal intubation,
try to notice the chest movement with serveral respiratory cycles and discard false positive strathosphere sign.
Fig. 11
Abscence of power slide
Abscence of laminar enhacement in the power doppler signal.
Some artifacts can be obtained if the patiet breaths heavily but the doppler enhancement doesn't have a laminar morphology.
Quiz
81 year old male with dysphea and chest pain.
Normal ECG and cardiac enzymes.
--Thoracic USG--
Left hemithorax zone I = Fig. 14, M-modeFig. 17
Right hemithorax zone I= Fig. 16,
M-mode Fig. 18
DIAGNOSIS??????
CT= Fig. 19





